This 59-year-old gentleman presented with acute occlusion of left radiocephalic fistula. He is a known case of chronic renal disease on maintenance haemodialysis. His dialysis was due for a few days and needed urgent access. He was referred for either salvage the fistula or create a new access for dialysis.
An ultrasound scan of the fistula revealed complete occlusion of the venous segment from the anastomosis. The venous segment from the anastomosis, however, taking a sharp U turn downwards and was quite difficult to access anatomically. Still the case was discussed in detail with the Patient’s family who wanted to salvage the fistula if possible knowing that it may be a futile exercise compare to creating a new access as a PERM cath placement suggested to avoid this procedure.
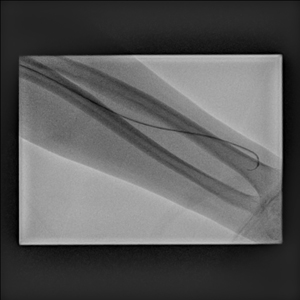
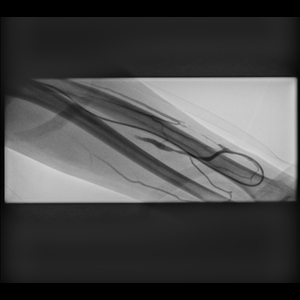
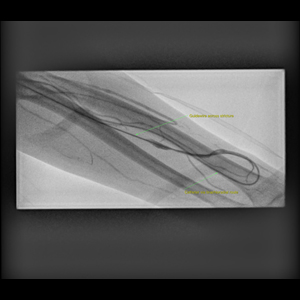
After careful consideration it was decided to start from the venous approach as U turn of the venous segment maybe more approachable from this side. Taking all aseptic precautions, initially in the distal draining cephalic vein near elbow, 6 Fr. sheath placed but all attempt to cross the fistula from the venous side through this route completely failed. After trying for sometime, it was decided to try from the radial approach which also failed as the sharp turn at the anastomosis could not be negotiated using any wire or catheter combination. It was then from the brachial route (puncture at elbow) fistula was accessed and a 5 Fr. sheath placed. Using catheter and wire, the anastomosis was negotiated and access gained into the venous segment. However, the balloon failed to track and only reached up to the U turn of the venous segment from the arterial side. All manipulations to take it distally failed , so was plastied here. From the venous approach the rest of the segment dilated in its entire course and thus a partial recanalisation of the entire segment could be achieved. The fistula started showing thrill and good flow on Doppler examination on table, so procedure was stopped as we could achieve desired result partially.
However, during haemostasis there was massive bleed from the brachial side, so a long compression was given which obstructed the venous outflow as well (as the both punctures were made nearby at the elbow) which after some time resulted in complete thrombosis of the venous segment with complete loss of thrill.
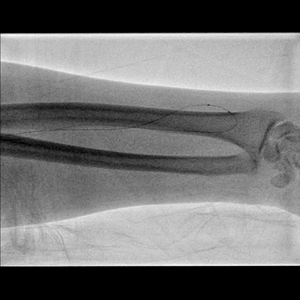
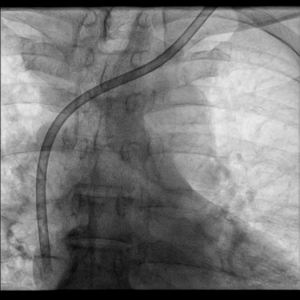
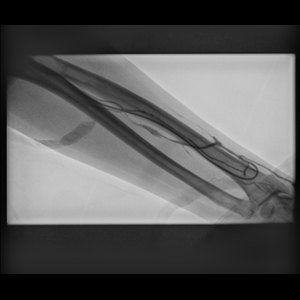
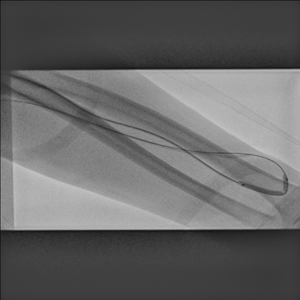
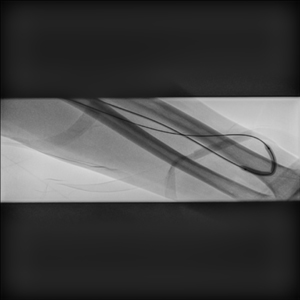
Next day, a Doppler examination showed complete occlusion of the draining venous segment which is distended with acute thrombus. Patient needed urgent dialysis with serum potassium was rising including creatinine, urgently a PERM cath from the left side placed. The case was again discussed as the options are quite limited and this time we decided to go for the thrombolysis of the venous segment which is acutely thrombosed. Next day, an access was taken distally in the arm& a 6-French sheath placed in draining venous segment. The anastomotic stricture was crossed using wire which was easier this time than previous time as the entire segment earlier balloned. Using 4 and 6 mm balloon the entire anastomotic and the venous segment was dilated. Contrast injection showed complete thrombosis of the venous segment with no outflow here. As the flow restored from the anastomosis we have started catheter directed thrombolysis of the entire segment. After 1 hour of thrombolysis with 10 mg of rTPA, the segment opened up quite well and thrill with venous flow started. The thrombolysis was continued for 18 hrs. and then it was stopped. On Doppler, the entire anastomotic segment completely opened up including excellent flow establishment in the venous segment.
Thus the AVF could be salvaged and later on dialysis was started from the fistula.
Note: At the AGHL, we are doing these complex fistula salvage procedures very often including the procedure for central venous obstruction and other venous issues for the dialysis access for long. However, this is possibly the first case of our where a combination of multiple access, plasty and thrombolysis was used successfully.