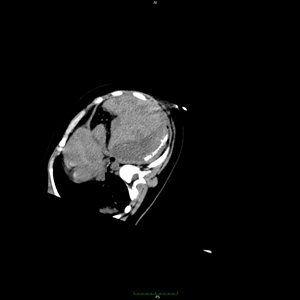
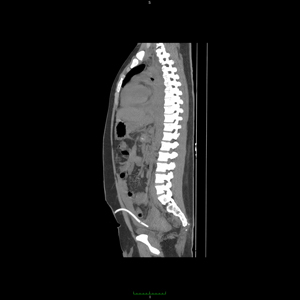
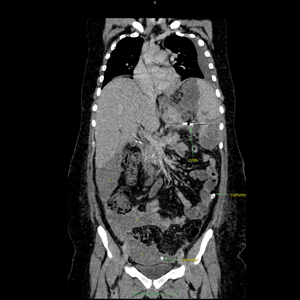
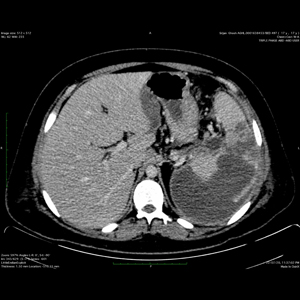
This 17-year-old boy presented in an outside hospital with significant pain in left upper quadrant of abdomen for few days. He is a known follow up case of chronic calcific pancreatitis, diagnosed about 5 years back following cholecystectomy. On presentation, his Serum lipase and amylase levels were found elevated and was diagnosed as a case of recurrent acute on chronic pancreatitis. However, he was found to have distension of abdomen, recurrent decrease in blood pressure with decrease in haemoglobin level. Several units of transfusion given. His oxygen level was fluctuating. Despite all conservative measurement when he was not responding, subjected to a triple phase CT scan of upper abdomen which showed huge amount of haemoperitoneum associated with branch pseudoaneurysm of splenic artery from the lower polar region. A huge perisplenic collection also noted along with chronic splenic vein thrombosis, decompressing via large amount of hilar collaterals towards the linogastric reasons , together with mild changes of pancreatitis at the tail area. Changes of chronic calcific pancreatitis also noted but the MPD not significantly dilated.
He was brought to us with these findings alongwith request for a splenic artery embolisation as they wanted to avoid splenectomy in this acute setting. On presentation,Covid RT-PCR test was done which was negative and then was taken up for an emergency embolisation of the splenic artery pseudoaneurysm.
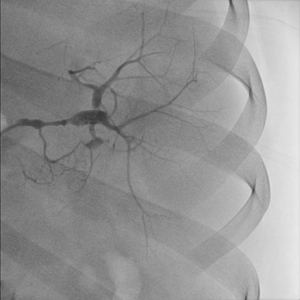
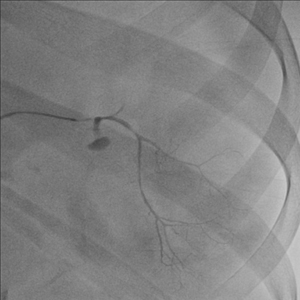
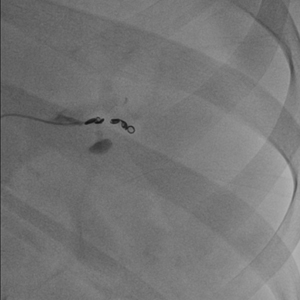
Using right femoral arterial access , 6-French sheath placed and the splenic artery was cannulated with 5-French C1 catheter. Contrast injection show well defined lobulated pseudoaneurysm from the lower branch of the splenic artery. The branch was occluded using coils & gelfoam as per protocol. One of the coil seen displaced into the upper branch origin as well.Gelfoam also was injected into the smaller nearby pancreatic branches to avoid any recanalisation of the branch. Post-procedure distal occlusion of the splenic artery and its lower polar branch observed but good recanalisation and reconstitution of flow especially via right gastroepiploic branch observed with complete preservation of flow to the splenic parenchyma.
He was shift it in ITU for observation where from the next day onwards he has started having high spikes of fever which was not responding despite changing to higher antibiotics. An ultrasound scan carried out, showed huge amount of collection in the peritoneal regions with organised collection in the sub and perihepatic region. Liquefied collection in the left perisplenic, pelvic and paracolic regions observed. An ultrasound guided large bore drainage catheters placed in the left paracolic region and in the pelvis.
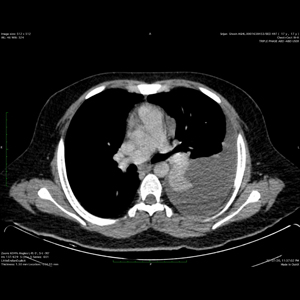
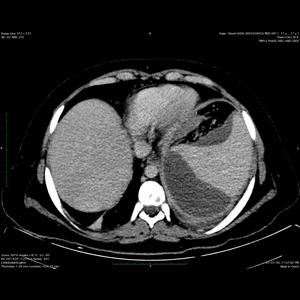
Despite good drainage, the patient continue to have high fever and getting sicker by day. Surgical referral was done but surgery was refused in this condition & conservative management suggested with higher antibiotics. A CT scan with contrast of the abdomen and chest done which showed huge amount of left pleural effusion and lung collapse alongwith large amount of collection in the perisplenic , peritoneal and other reasons. Large collection from the lower pole of his spleen seen communicating with the left diaphragmatic massive haemorrhagic collection and suspected of having infection there. He was also having decrease in oxygen saturation and significant pain during the respiratory movement on left.
Antibiotics changed again what is still not produced any result. So, a CT guided catheter drainage of left pleural effusion and a large bore catheter into the splenic collection placed and extended up to the left subdiaphragmatic region. Following this, the left paracolic and pleural collections resolved and the catheters were removed. Small amount of drainage which were haemorrhagic, continued coming out from the spleenic and pelvic catheters, so they kept in situ.
His blood culture grown E coli and sensitive antibiotics were started but fever was kept coming although the white blood cell count has started decreasing. His procal still was high and at least 2-3 of spikes of high grade fever recorded everyday. After a few more days of conservative treatment a PET CT scan of whole body performed to look for any other source of infection. This examination showed the perisplenic area with high FDG avidity suggestive of infection where no liquified collection was present. Surgical referrals, however, given several times but as there was no definite area to be treated, surgery was refused in presence of splenic vein thrombosis with large amount of collaterals and previous pancreatitis.
After a few more days of observation, he was shifted to ward and continued on higher antibiotics. The splenic and pelvic drainage continued, so they kept in situ. As his WBC count and procal were coming down but he still continued having fever, so decided to discharge him on IV antibiotics for long-term along with the catheters. A 5-French double lumen power PICC line placed via left basilic vein and he was discharged with 2 catheters in situ alongwith course of antibiotics to be given. His splenic and pelvic catheters were subsequently removed and as the fever responded with long-term antibiotic, his PICC line was removed as well.
He is doing well even after 3 months until now there is no episode of fever or any decrease in haemoglobin. A follow up scan is due but due to raging pandemic still not performed. Ultrasound examination of the abdomen showed no more liquefied large collection.
Thus, together team Apollo able to manage a complex case of intraperitoneal pseudoaneurysm rupture and Massive hemoperitoneum non-surgically, complicated by severe superadded infection in the setting of chronic calcific pancreatitis alongwith splenic vein thrombosis. His hemoglobin and BP were stable throughout post procedure and no more episode of any bleeding recorded.