A 54 year male with the congenital slow venous formation of the left lower limb presented to this hospital with a history of spontaneous midshaft fracture of left femur requiring fixation. He earlier went to another hospital where attempt of fixation resulted in a massive torrential bleeding from the incision site from the vascular malformation having grossly dilated superficial veins.
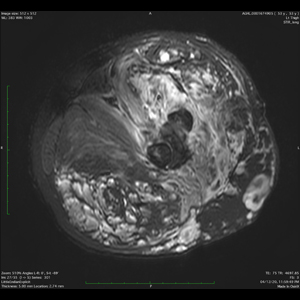
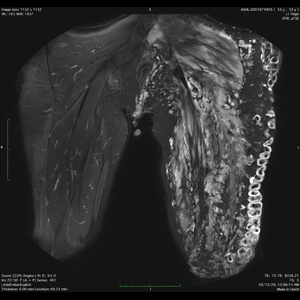
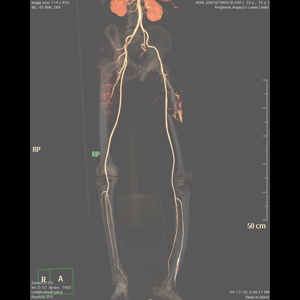
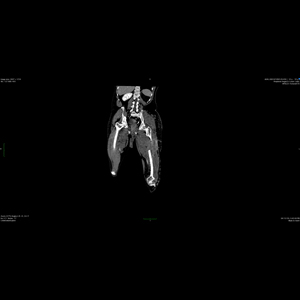
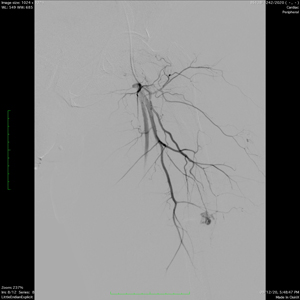
On presentation, a CT angiography of left lower limb performed which showed vascular extravasation from a tiny branch of left profunda femoris artery at the fracture site and diffusely dilated superficial veins subcutaneously along the lateral aspect of the thigh. MRI of thigh performed showed extensive vascular malformation involving nearly all the muscle groups of entire left lower limb extending up to the left side of the scrotum with few grossly dilated tortuous veins superficially.
Case was discussed in the detail. Patient needed fixation of the overriding fragments of fracture femur after reduction but the vascular malformation would have bleed profusely during the operation. As a minimal intervention, external fixator application was considered with multiple pins but before that vascular malformation needed some management. After discussion, patient was taken up for the embolisation of the deep femoral branch which was giving extravasation at the fracture site followed by sclerotherapy of the superficial veins at prospective insertion site of the pins of fixator.
Through right transfemoral approach under local anaesthesia, the left sided common femoral artery and its profunda femoris branch super selectively cannulated, the injection of which showed active extravasation going to the venous side, progressively embolised with gel forming solution followed by a coil leading to its complete occlusion. Before starting of the procedure, all the prospective sites of pin insertion marked. Below those marks, ultrasound-guided puncture of the dilated veins was done and sclerosants were injected. After completion of the procedure, the patient was shifted to Ward. Next day, he was taken up for the operation where the reduction of the fracture and external fixator applied with a small amount of blood loss.
Thus a complicated fracture femur with vascular malformation is managed well combinedly with judicious use of interventional procedures. Internal fixation of this fracture was not possible as long standing vascular malformation lead to the weakening of the bones and the medullary cavity was very thin.