What is PTBD ?
Percutaneous transhepatic biliary drainage (PTBD) is the process where a trained interventional radiologist places a catheter in the dilated or obstructed biliary system percutaneously through the liver parenchyma to drain out the bile and thus reduce the jaundice in cases of obstructive pathology.
However, the patient will have a bag lying outside the abdomen in which the bile will be collected, requires emptying everyday. This results in loss of bile salts and pigments with some essential minerals as well.
The process of crossing the obstruction and placing the tube across the narrowing to drain the bile inside the body into the duodenum, called internalization or internal-external drainage of the catheter. Internal- external drainage if functions well, the tube will be detached from the bag and only tip of its lying outside.
Frequently, this is followed by placing a metallic tube or stent across the narrowing specially in cases of malignant or cancerous disease to facilitate internal drainage of the bile where the stent facilitates normal drainage in the duodenum through its normal pathway and the catheter will be removed.
How it is done ?
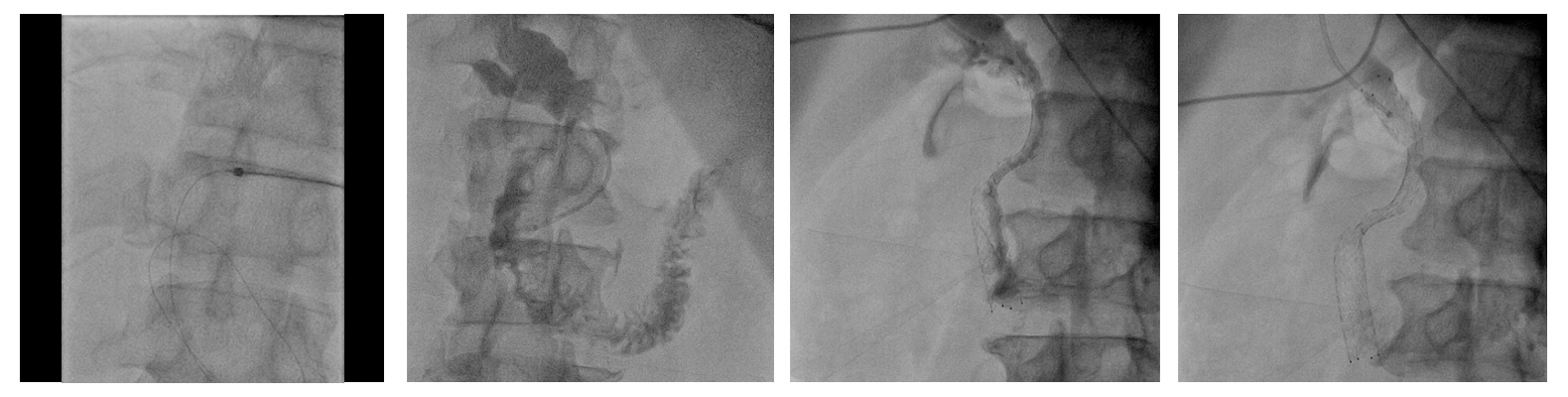
Usually under ultrasound guidance taking all aseptic precautions and under local or general anaesthesia, the interventional radiologist using a thin long needle, punctures the choosen peripheral biliary duct, taking care not to damage the adjacent vascular structures, which might result in significant bleeding. Once the needle gets into the system and bile starts coming out, usually places a wire under fluoro guidance into the system over which a sheath advanced. Using different techniques, guidewire with catheter combination, he enters into the main or larger duct to be drained and usually places a catheter for initial drainage. This catheter is then fixed to the skin and connected to a bag outside the body for drainage of the bile.
Sometimes in same or next sitting, using same pathway with different catheter and guidewire combination, IR tries to bypass and cross the narrowing in the system and places a catheter across it to drain the bile through its normal pathway into the duodenum called internalization. However, if he able to cross the narrowing, at times especially in cases of malignant obstruction due to cancerous causes, it is preferable to place a metallic stent across the narrowing which keeps that channel open for a longer time and gives inward drainage of the bile after which catheter can be removed on suitable time.
In cases of benign biliary stricture, nowadays at times, retrievable metallic stents placed to facilitate the drainage and keep the system open for longer duration till the pathway becomes open and patent for adequate drainage, upon completion of which stent can be removed percutaneously. In cases of periampullary or pancreatic head cancers or cancers of the lower CBD, it is possible to place a covered stent across the narrowing which prevents the tumor ingrowth in the stent and keep the passage patent for longer duration of time.
Endobiliary RFA
In some patient, it is possible to ablate the tumor with delivery of radiofrequency energy at the site of narrowing which helps in keeping the stent patent and functioning for the longer duration of time.
Who should do it?
A very well trained interventional radiologist who is conversant with biliary anatomy and pathology with experience of doing these procedures should do it.
Complications :
As the procedure is done directly through the liver, it is always having dreaded complication of significant bleeding through the puncture or inside. The bleeding at times may be very severe and fatal although very rare in occurrence as the trained interventional radiologist usually tries to avoid the vascular structures near the bile duct. At times if bleeding is severe, other procedures like embolization to stop the bleeding may be needed. Usually it settles with the conservative treatment where transfusions and other therapies will be required.
Another significant and feared complication is severe infection or biliary sepsis which if uncontrolled can again cause loss of life. However, usually all these patients placed on the antibiotic therapy and drainage of infected bile result in great recovery.
Hospital stay:
Usually one to three days. After biliary drainage, patient can be discharged with catheter in the very next day. Whereas in cases of stenting, it is preferred to keep the patient in the hospital to see the progress.
What are the indications:
Obstructive jaundice of any pathology, may require PTBD especially in cases where ERCP cannot be done like postoperative status and where ERCP fails. Usually after previous operation like hepaticojejunostomy or partial gastrectomy, there is no access route for ERCP where PTBD is preferred, the only option to reduce the jaundice. In cases of ERCP failure, also PTBD should be done as soon as possible to prevent any possibility of infection.
In some cases preoperatively, PTBD is more preferred than ERCP as it creates less scarring and inflammatory changes around the surgical site especially in the cases of carcinoma in the head of pancreas or periampullary Ca.
One stage or two stages preferred:
The PTBD with biliary stenting can be done as a single stage procedure but sometimes these get complicated with severe sepsis especially where the obstruction is long standing and results in severe morbidity with at times mortality. So for longstanding especially in the lower end obstruction of the biliary system, a two stage procedures is preferred where in initial stage the bile is drained and once the jaundice reduced or patient improves, in second stage stenting can be done.
Can it be repeated:
In cases of recurrence of obstruction or jaundice, PTBD can be repeated especially in cases of obstruction of the proximal CBD or periampullary region. Benign biliary strictures which usually results in repeated cholangitis and jaundice also requires multi system PTBD at times depending upon the level of strictures and their involvement.
The anatomical considerations:
Liver secrets bile which collects through the tiny ductules which joins to form the larger ductules or ducts here. For anatomical purposes, liver divided into several segments. All segments are drained via their respective bile duct and supplied by hepatic arteries with portal vein. Together these three structures form porta hepatis. These segmental bile ducts, join on right side to form right anterior and posterior ductal system which further joins to form larger right hepatic duct. Similarly on left, they form segment II and segment III ducts which joins to form the left hepatic duct.
The segment IV duct either joins the right or left system but usually to the left system. The right and left system then joins to form the common hepatic duct and their joining point known as hila. This common hepatic duct then comes out of the liver and joins the gallbladder duct or cystic duct to form the common bile duct or CBD which drains into the duodenum via an opening at ampulla. Here before opening at the ampulla, it usually joins the main pancreatic duct or the duct which drains the pancreatic juices to the duodenum.
This common channel called as the common pancreatobiliary channel. Obstruction anywhere in the system, results in swelling of the rest of the area known as dilatation of the biliary radicles and ducts. Obstruction at the lower end or the lower CBD usually caused by carcinoma of the head of pancreas or periampullary CA here along with lower end of CBD cholangiocarcinomas. Blockage anywhere from the ampulla to the hila results in dilation of the entire system but can be drained by a single biliary drainage catheter.
However, with the involvement of hila, the right and left system usually gets separated and that is termed as isolation of hila. This hilar isolation is of supreme importance and has to be properly diagnosed for proper planning of the procedure. The progression of the tumor beyond this point towards the right or left results in separation of the more ducts. This separation of the right anterior or posterior ductal system known as subsegmental isolation. The more peripheral the disease with subsegmental isolation, the issue becomes more complicated. As usual, if it goes beyond the main right or left hepatic duct, the drainage procedure becomes quite difficult and complicated as well.
In those circumstances, the intervention radiologist usually chooses a system which drains the larger volume of the liver and it usually suffices in cases of malignant disease. However, a patient having infection known as cholangitis or cholangitic abscesses, the intervention radiologist may be forced to do drainage of the one or more ductal system as the system with the infection has to be drained otherwise patient will not get any symptomatic relief despite adequate drainage of the bile through the other ducts.
Sometimes after drainage of one of the system via ERCP by the gastroenterologist, the undrained system in cases of hila or subsegmental isolation, gets infected results in severe cholangitis which needs immediate drainage through the PTBD for relief of the symptoms and at times to salvage the patient as the cholangitis is one of the most severe form of infection which if continues can result in loss of life. In those cases after PTBD, the second step usually becomes very difficult if a metallic stent is placed via the ERCP, as going through the previously placed metallic stent and the narrowing becomes very tough. At times the IR needs to do serial dilatation with the balloon through the metallic stents to make a passage via it. After that he places a metallic stent through the stent and this is known as stent within stent. Sometimes multiple stents placed to make the entire system working in patient known as hilar reconstruction.
Treating benign biliary stricture:
Benign biliary strictures (BBS) dealt completely differently than the malignant obstruction as the patent’s life expectancy is more and it is a benign disease. This usually happens after surgery or repeated infection where the system is not significantly dilated. Although the patient is very symptomatic especially during the episodes of severe infection gets cholangitis or significant rigors having fever and increase in the liver enzymes with bilirubin. In those cases, multiple ducts which are involved needs to be drained and then sequential dilatation after a gap of three to four weeks of the strictures done with balloon or larger catheter and the catheters after internalization kept in situ for the internal drainage. This sometimes requires one or more years to replace till cholangitis settle and the strictures dilate to a level not resulting in any more bouts of cholangitis or inflammation. At times, now a days as mentioned earlier retrieval stents placed to keep the system widen which can be taken out later once the ducts attends a good calibre or widened up.
Intrahepatic stone removal:
Sometimes the biliary system gets loaded with the formation of stones in them which are not possible to drain via the ERCP or endoscopic route. In those cases, after PTBD the tract serially dilated and then through the percutaneous route can be serially taken out. At times they require cholangioscopy for direct visualization and removal. Sometimes, they need breaking of the calculi inside and crushed and then swiped into the duodenum or can be taken out percutaneously. At times ESWL also perform in places where it is available to break the stones in small particles which can be drained through the stricture into the duodenum.
Can it produce survival benefit in cases of malignancy:
Biliary stenting or drainage in a patient of malignant biliary obstruction is usually a palliative procedure which does offer substantial benefit. However, usually a palliative procedure and does not treat the primary pathology. Thus not providing any great survival benefit. However, this prevents severe biliary infection resulting in sepsis with loss of life or from developing of hepatic encephalopathy or other.